
This three-part series looks at brain-computer interfaces: what they are, what they could become, and the implications of connecting our brains directly to computers.
In part two, we see how these devices are being used today and some of the limitations that engineers and scientists still need to overcome.
A person living with amyotrophic lateral sclerosis (ALS) experiences the gradual death of motor neurons – the parts of the brain that control our movement.
Over time, their muscles weaken and atrophy. Depending on which limbs are affected first, the person may start tripping and stumbling, or find their hands fumbling with everyday objects.
Eventually the person will stop being able to walk or use their hands. Speech becomes unrecognisable, then impossible, as does chewing and, finally – fatally – breathing.
In part one of this series, we touched on the potential for brain-computer interfaces (BCI) to connect our brains with artificial intelligence, navigate virtual worlds, and augment the human experience far beyond our current comprehension.
But the reality of BCI technologies today is more prosaic yet no less miraculous in the way it changes lives.
In late 2021, Philip O’Keefe, a man living with the severe neurodegenerative disease ALS, sent a tweet using the Twitter handle of Thomas Oxley, CEO of BCI company Synchron that spun out of the University of Melbourne.
“Hello, world!” Philip said. “Short tweet. Monumental progress.”
More than a year earlier, an 8mm electrode array called a stentrode made its way up Philip’s jugular vein and into a blood vessel in his brain. Here it expands against the vessel walls so it could intercept neural activity.
For a brief half an hour in the days leading up to Christmas, Philip got to tweet just like everyone else.
“No need for keystrokes or voices,” he said. “I created this tweet just by thinking it.”
no need for keystrokes or voices. I created this tweet just by thinking it. #helloworldbci
— Thomas Oxley (@tomoxl) December 23, 2021
The purpose of stentrode is to offer people with a way of once again performing what Synchron CTO Nick Opie calls “activities of daily living”.
Writing emails and sending tweets are a natural part of these daily activities, but so are the kinds that we take for granted, like online banking and shopping.
“When we started out about 10 years ago, what we wanted to do was have really good information from underneath the skull, but get there in a way that doesn’t require invasive surgery,” Opie told Information Age.
“So, we took a lot of advice from what’s happening in the cardiovascular space and figured out that there are some really nice blood vessels that we can use to access the same part of the brain, the motor cortex, that other technologies use.”
Being in control
Once the stentrode is in place, it transmits data down through a wire and into a small receiver on the chest. That receiver can be used to wirelessly control a computer.
It’s important to understand that the control doesn’t happen by pure intention – Philip didn’t merely think “send a tweet saying ‘Hello World’”, and off it went.
Rather, he navigated a user interface except instead of moving a mouse cursor with his hand, he used his mind.
Current BCIs tend to be implanted in or around the motor cortex because it’s a location that can offer strong, repeatable signals which can be interpreted as specific inputs for a computer.
In an abstract sense, it’s not much different to how we currently use computers: you think about the action you want to make and then your brain send signals (via the motor cortex) to your hands and fingers to move the mouse, to tap on an icon, or type on a keyboard.
Just imagine removing the mouse, the screen, and the keyboard from the equation.
The problem is that, while mice, touch screens and keyboards are fairly interchangeable, everybody’s brains are different.
“We've implanted seven stentrodes and we're just starting to really figure out what the best way is of interpreting this information and using it reliably to control things,” Opie said.
“For one gentleman, he would think about moving his left leg, and that would give a really nice signal. He obviously couldn’t move it, but every time he thought about doing that, it would equate to a switch that he could use to do a mouse click, for example.”
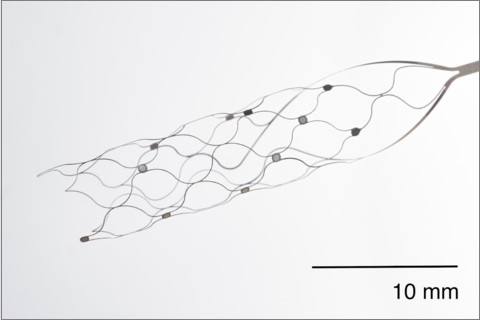
The stentrode gathers brain signals from the walls of a blood vessel. Image: Synchron
A person’s ability to send specific thoughts is also dependent on their former hobbies and habits. If you used to play the violin, you might find it easier to think about using your hands to control a computer with your mind, for example.
This creates serious limitations for how generalised BCIs can currently be.
Not only does the patient need training to think about moving parts of their body that are paralysed so they can do something completely different (like clicking a mouse by thinking about moving their leg), but computers also need to be trained to recognise those specific types of brain activity when they happen.
The result is a highly personalised product that tailors itself to the user’s specific brain function.
As such, the idea that Elon Musk’s Neuralink could do something as complex as “save and replay memories” using devices that are implanted en masse seems far-fetched.
Further advances in machine learning and artificial intelligence will no doubt help make it simpler to on-board BCI patients in the future, but for now even that has its limits.
The strict regulations around health technology, like implants that go in or near the brain, have ramifications for algorithms that adapt to users.
“We can do that offline,” Opie told Information Age. “But there’s still questions about whether artificial intelligence being used in an online system is acceptable to the FDA [US Food and Drug Administration].”
Synchron has been approved by the FDA to conduct human trials – an important regulatory and experimental hurdle to overcome before the product goes to the wider market.
“When you think about it, the FDA needs to approve software to say it is safe to use. So, if you have an AI or machine learning-based algorithm that changes over time, the algorithm you've got at the end of the day might not be the same as the one that they approved to start with.”
Physical limitations
Stentrode aims to strike a nice balance between minimally invasive electrodes placed on the outside of the skull – which have a low signal fidelity – and highly invasive surgeries that see patients’ skulls cut open and devices implanted directly onto brain tissue.
“The body is very good at rejecting everything we do to it,” Tara Hamilton, the principal scientist at Australian sensor technology company Cuvos told Information Age.
Earlier in her career, Hamilton worked for Cochlear – the Sydney-based biotechnology company that revolutionised hearing aids with its cochlear implants.
These devices comprise microphones that pick up sound, processors that filter out noise and amplify speech, and transmitters that send the signal to a device under the skin which decodes it and communicates with the cochlear nerve that, in turn, sends signals to the brain.
Mass adoption of cochlear implants shows the appetite for technological solutions to problems with our all-too-human hardware and the ability to turn the technology into a business (Cochlear made a $277 million profit off $1.6 billion in revenue in the 2021-22 financial year).
“My first job at Cochlear was in quality and I used to get back the devices that had failed,” Hamilton said.
“These devices had been implanted for a few weeks and then a kid might have fallen over, hit their head and damaged the implant – the kid was fine, the implant not so much.
“What was really interesting was seeing how much scar tissue there was and how big cells, called macrophages, had started to form along the electrode lead.
“Anything that’s not you, your body will just completely reject. So, the biggest barrier in terms of interfacing is always the human body.”
Enter the world of materials science. It’s worth noting at this point the interdisciplinary nature of BCI research and development. Computer science, engineering, neuroscience, medicine, psychology, robotics, and materials science all converge on the world of BCI.
Engineering the right components from the right materials is, for Hamilton, the best way to overcome our body’s in-built rejection mechanisms.
Sending signals to the brain is an important step in building BCIs as a direct mode of interacting with the brain and it already has real world applications, such as for managing the tremors caused by Parkinson’s disease.
In this case, deep brain stimulation sees electrodes implanted onto brain tissue where it delivers small impulses that limit tremors.
There has also been research into devices that can bypass the eyes to deliver images directly to the brain, giving people living with blindness sight again.
Consider the implications of what it could mean to not only control computers with your mind – a one-way process – but have the computer then respond straight into your brain, creating images, sounds, or feelings inside your mind.
But as the research extends from capturing (reading) brain signals to sending (writing) them, physics – not just biology – gets involved.
“When you have a current and you’re trying to push it through a smaller and smaller electrode to make ever finer contact, the resistance of that contact goes up exponentially,” Hamilton told Information Age.
More resistance means higher voltages and currents – neither of which are desirable when setting up wires that send signals to the brain.
“You have to think about how to make it so you’re not hitting the brain with too much current and you’re not putting artificial substances in there that will eventually corrode and cause other problems,” Hamilton said.
“The big thing with deep brain stimulation is that you have to put so much current in to get such a small response.
“For the people that get it, it’s very effective, but you’re doing damage, so it needs to be really necessary in order to be put in – it’s not something you would have as a recreational type of device.”
In the final part of this series, we will look at what happens when implants become obsolete, and reflect on the legal, ethical, and philosophical implications of developing and using BCIs.